
Kirsten’s case is discussed at a multidisciplinary team meeting. Present are a consultant cardiologist in Adult Congenital Heart Disease (ACHD), consultant cardiac surgeons specialising in CHD, ACHD nurse specialists, a cardiothoracic anaesthetist, paediatric consultant cardiologists, and sonographers.
The team review Kirsten’s case and look at her recent test results and images. Because Kirsten had symptomatic changes, functional deterioration on her cardiopulmonary exercise test and an increase in the size of her ventricle, the team decide that the timing is right to proceed with a pulmonary valve replacement.
Right Ventricle to Pulmonary Artery valved conduit
In patients with ToF, reparative surgery can either involve widening the native right ventricular outflow tract (RVOT) or, in severe cases where this is not amenable, a valved conduit can be inserted. This involves a prosthetic tube and valve being placed between the right ventricle and the pulmonary artery. This replaces the native RVOT.
Pulse point
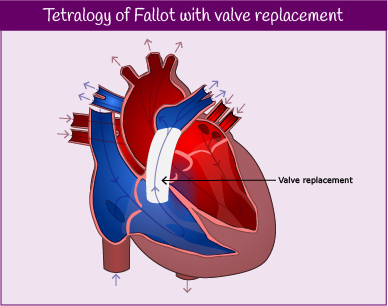
Valve replacement
Deciding when is the right time to carry out a valve replacement in patients with congenital heart disease can be very difficult. Valve replacements often require replacement at about 10-15 years and patients require repeated procedures throughout their life. It is, therefore, important to balance the need to replace a valve and prevent further dilation or dysfunction of a ventricle with consideration of the number of possible future interventions.