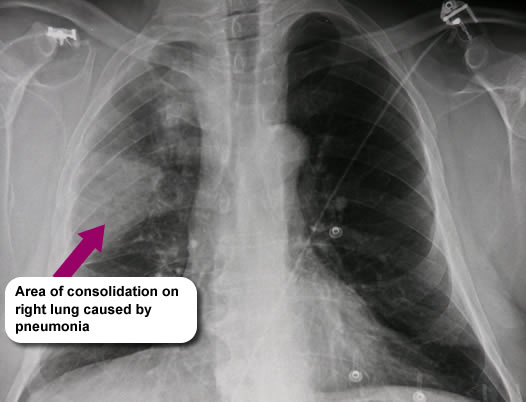
Twenty-four hours later, whilst carrying out a routine set of observations the nurse noticed that Mrs McGinty had a raised temperature of 38.1°C and that she was sounding chesty. A chest X-ray was carried out and she was diagnosed with a chest infection.
Dyspnoea
Refers to a shortness of breath, difficult or laboured breathing with an increased respiratory rate (RR). A normal respiratory rate is 12-16 breaths per minute.
Mrs McGinty has a RR of 25 breaths per minute which is causing her to feel anxious.
Pallor
Patients with infection may appear flushed or pale. Mrs McGinty is hot and clammy.
Blood gases
Arterial blood gases (ABG) are measured using blood from an artery (usually radial artery at the wrist) and test the acidity and levels of oxygen and carbon dioxide in the blood.
Mrs McGinty’s ABG results are as follows (normal values given in brackets)
- SaO₂ – 85% (≥95%)
- PO₂ – 8.5 KPa (11-13)
- PCO₂ – 7.5KPa (4.6-5.6KPa)
- H⁺ – 40mm/l (35-45mm/l)
- HCO₃ – 30 (22-26)
- PH – 7.42 (7.35-7.45)
Mrs McGinty’s results are typical for a patient with COPD and an acute chest infection.
Breath sounds
Air entry into the lungs can be assessed by listening to the chest wall with a stethoscope. Normal breath sounds (BS) are:
- heard more prominently at the top of the lungs
- soft and muffled
- ratio of normal expiration to inspiration is approx 1:2 during relaxed breathing
Mrs McGinty has reduced BS throughout the left lung as a result of shallow breathing and has bronchial breath sounds on auscultation of the right lung. Bronchial breath sounds are:
- loud and harsh
- heard throughout inspiration and expiration
Bronchial sounds may be caused by:
- consolidation – as confirmed by her chest X-ray
- areas of collapse
- pleural effusion
Cough
The patient’s cough is often unproductive in the early stages of a chest infection. Patients with hemiparesis can experience difficulty in expectorating secretions due to paralysis of the trunk musculature. Also the presence of apraxia may interfere with Mrs McGinty’s ability to voluntarily cough.
Mrs McGinty has a moist cough and is producing small amounts of secretions.
General malaise
Before her admission to hospital Mrs McGinty had been lying immobile on the floor for a period of time, was dehydrated and malnourished.
Mrs McGinty should be closely monitored and her vital signs regularly recorded.
Pyrexia
Most people with chest infections have a fever. Mrs McGinty has a temperature of 38.1 ºC.
Aspiration
Aspiration is the breathing of foreign materials (usually food, liquids, vomit or fluids from the mouth) into the lungs. Stroke patients commonly present with dysphagia and as a result may need to be managed as ‘nil by mouth’. Even when a patient has a nasogastric tube in place they may still have problems controlling their saliva and secretions which can then enter the lungs.
Mrs McGinty’s swallow screening assessment showed that she was at potential risk of aspiration and she is now nil by mouth.
Page last reviewed: 20 Apr 2021