There are numerous variations in supports available for hemiplegic shoulder pain. Their aim is to re-align the shoulder complex into a normal position.
The success or failure of these supports is often associated with:
The complexity of the design which affects application
The patient’s compliance with wearing the support
Staff compliance with the support wearing schedule
The patient’s size – off-the-shelf designs may not be suitable for all patients
The extent of the paresis and extent of the patient’s involvement in physical rehabilitation
Strapping can be used as a custom made solution for re-alignment of the shoulder which may be effective in reducing pain in the acute setting. Clinician judgement and care must be exercised in deciding the length of time of the application as there is a risk of skin breakdown.
The photographs below show shoulder strapping being applied:
Electrical Stimulation (ES): is a treatment modality which uses electrodes applied to the skin which stimulate the muscles to contract. It has been shown that ES decreases subluxation and shoulder pain in post acute care following stroke. These benefits may not be maintained beyond 6 months.
Pain is a presenting feature that may interfere with rehabilitation and cause distress to people after stroke with as many as 42% reporting some painful experience. There is still a general lack of knowledge about the way pain is perceived and reported by people with brain damage in general, and stroke in particular and it is often an overlooked symptom not well addressed in clinical care.
Analgesic intervention should match the nature and severity of the pain. There will be locally agreed protocols on the prescription of analgesia which usually follow a ‘staged’ management approach similar to that below:
To achieve the optimal analgesic affect prescribed medications should be:
Appropriate to the pain described
Given regularly and as prescribed. A loading dose may need to be established and maintained for the drug to be able to work effectively
Sufficient to enable the patient to engage in physical rehabilitation
Discussed regularly within the multidisciplinary team
NB: NSAID’s are not recommended for use in post stroke care due to a potential increased risk of bleeding if taken with antiplatelet therapy.
Patients should be made aware of the potential side effects of the medications being administered and should be closely observed for any signs of these adverse effects.
There are a number of pain assessment tools available, some of which are aphasia friendly.
Alternative methods of administration e.g. via nasogastric tube need to be considered for patients with dysphagia who cannot take medications orally.
Other interventions may include injecting the shoulder with corticosteroid or anaesthesia. In some cases hypertonus can be treated with injections of botulinum toxin but this treatment option is unusual in the early stages of stroke rehabilitation.
For more information
Feeding, nutrition and hydration following stroke: Medications
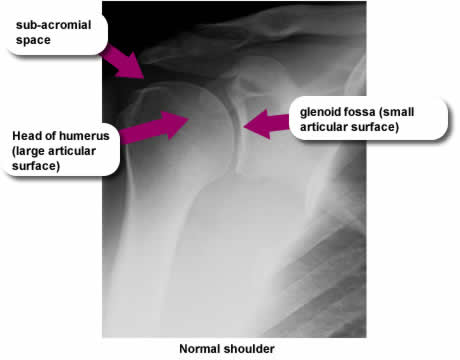
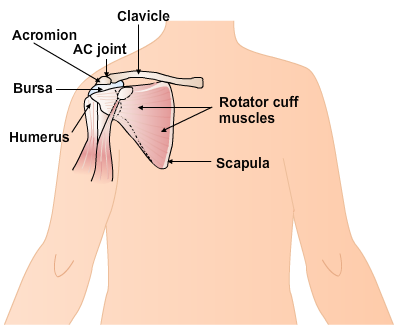
The integrity of the shoulder joint relies on muscular strength because as you can see left, the bony articular surfaces of the head of humerus and glenoid fossa differ in size to allow for a large range of movement at the shoulder. This results in a natural instability which means that the shoulder is at risk of dislocation and damage. Control of the range of motion at the shoulder involves a number of small muscles whose tendons pass between the moving bony surfaces. These may easily be damaged if the bony alignment is compromised.
Investigations
X-ray
Useful in identifying bony displacement and / or underlying fractures. A thorough clinical assessment will inform the best physical management, however in the presence of hemiplegia, precisely locating the anatomical structure involved is difficult as many of the diagnostic tests cannot be used. The presence or absence of subluxation can be determined by using palpation of the sub-acromial space.
MRI
Scanning has been used for diagnostic purposes but all imaging must be used with caution as similar pathological changes may be seen in people of a similar age who do not report pain.
Ultrasound
In the chronic intractable stages of shoulder pain ultrasound may be used to identify structures which may then be treated by injection with local corticosteroid.
On the morning after his arrival on the ward, the nurses report that Mr McTavish is complaining of pain in his left shoulder during routine care.
You know that Mr McTavish has a low-toned, subluxed left shoulder with reduced shoulder shrug and limited range of movement in his left upper limb. It was not clear exactly what happened at the time of his stroke, but given his previous golfing ability and the fact that he was enjoying this sport on holiday when he had the stroke, it is reasonable to assume that he did not have severe problems with the shoulder previously.
You have successfully transferred Mr McTavish to his chair and adapted it to enable him to maintain a good seating position. What other things should you now consider?
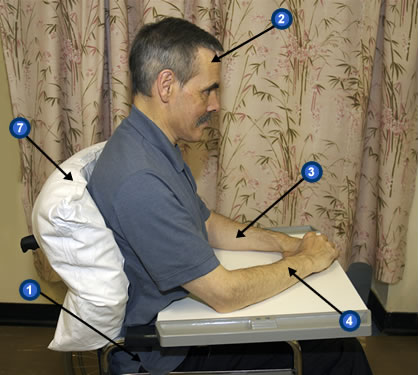
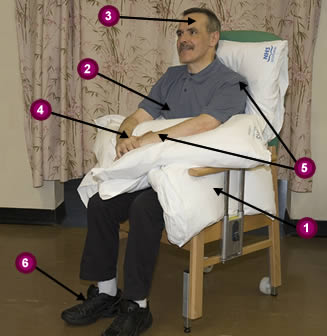
The following pictures show how careful positioning of Mr McTavish and the use of appropriate support (in this case pillows, lap tray and cushion) can influence his alignment.
Specific points to note:
Hips – central and at the back of the wheelchair
Head – central and eyes looking ahead
Left upper limb – supported by laptray
Right upper limb – supported by laptray and no longer required for balance
Footplates – correctly adjusted so that ankles, knees and hips are at 90 degrees which will help to reduce tone
Appropriate pressure relieving contoured cushion
Pillow used to ‘take up the slack’ in the wheelchair back in this case
NB: Consider making a referral for a specialist wheelchair assessment
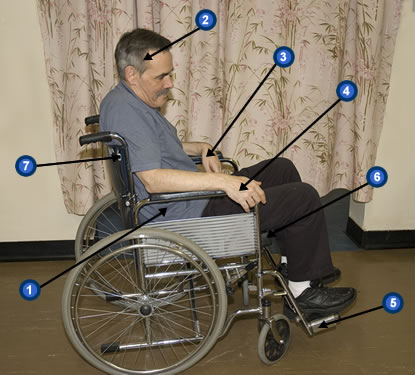
These pictures shows Mr McTavish who has left-sided hemiplegia and is unable to maintain a good sitting position in his wheelchair due to a lack of support.
Specific points to note:
Hips – not central and too far forward in wheelchair
Head – orientated to the right with eye/gaze deviation to the right
Left upper limb – increased tone
Right upper limb – required to help maintain his balance
Footplates in left hand photo are too high, causing increased pressure on sacral regions, in the right hand photo there are no footplates causing the patient to slip down in the wheelchair putting increased pressure on the thighs






 X-ray
X-ray