Often the most appropriate chair requires further adaption to achieve the optimum position for the patient. Unfortunately the only chair available on the ward is the green chair which will now require further adaptation to achieve an optimal seating position for Mr McTavish.
To assist Mr McTavish to achieve a good seating position, you must now select appropriate equipment from the following items.
To optimise seating and positioning multi disciplinary team working is important to establish the right chair and support.
Once you’ve had a go at figuring out the correct options for yourself, click on the item below to expand it and see what happens when Mr McTavish is put into each chair.
Compensations commonly develop when hemiplegia is associated with visuo-spatial inattention and when patients are unaware of their hemiparesis. Patients may generate excess activity in the non-affected side initially through a fear of falling, usually to the side that they perceive most easily, i.e. the unaffected side. This may result in the commonly seen “out of line/pusher syndrome” which is characterised by overuse through pulling or pushing movements or inappropriate balance/righting reactions. Movements and postures that we find difficult to rationalise may be perceived as entirely normal by the patient.
Pusher syndrome may be simply alleviated by providing adequate support and guidance on the unaffected side. Care must be taken in the rehabilitation of patients where muscle tone and alignment may be adversely affected by compensatory activity, although it may have to be accepted and modified in certain circumstances where a degree of compromise is unavoidable in achieving functional goals.
Mr McTavish has overuse of his right side, tending to grasp and fix on to supports. Initially he tended to push himself over towards the left side. He is learning that this does not help and is now starting to pull himself on to the right hip when sitting. His ability to align himself within his base of support needs to be addressed. He should not be encouraged to use the right arm for effortful function as this will increase asymmetry and tone on the left side and may affect his body schema and orientation.
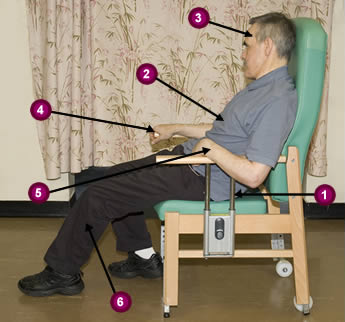
Figure 1. Out-of-line/pusher syndrome
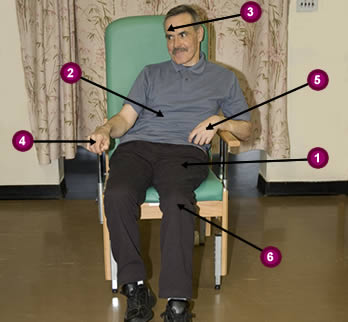
Figure 2. Fixing with right side
Pushing towards affected side with arm
Trunk side-flexed towards un-affected side
Head side-flexed towards un-affected side
“Pressure-bearing” rather than actively weight-bearing through affected hip
Head rotated to right
Pulling to right with arm
Weight distributed on right hip
Management plan- To reduce and control compensation strategies by:
Using base of support and positioning strategies to manage the unaffected upper limb (as well as the hemiplegic side)
Making appropriate functional demands to the level of recovery so as to prevent the need for compensations
Explaining to the patient the rationale for these management strategies to maximise compliance
Discussing management strategies with MDT to ensure a coordinated and consistent approach
The incidence of hemiplegic shoulder pain (HSP) has been reported as occurring in between 30% -65% of post stroke patients. With around 1/3 of patients developing HSP within 6 months of their stroke. The duration of this pain varies with around 65% of these patients reporting HSP for a number of months. See additional information for references and links to articles (PDF).
All stroke patients should be asked if they are in pain and this should be considered by the MDT to determine the nature and best management of any pain. Where a recommended treatment regime is designed, all staff should be aware of and contribute to this so as to ensure best analgesic control. This will enhance the ability of that patient to take part in physical rehabilitation.
It is important to identify the onset of shoulder pain at the earliest possible moment so that the most appropriate intervention can be initiated. The diagnosis can be made on the subjective report of the patient or, in the case of aphasic individuals, where facial expression or body language indicates pain either at rest or on passive movement. Remember that where joints are misaligned through abnormal tone, passive movements may cause pain due to a failure to give adequate manual support (not because there is damage to the shoulder). Subluxed (partially dislocated) shoulder joints should be handled with extreme caution.
Inattention/hemi neglect occurs when stroke patients do not attend to the affected side of their space/body. This is most usually seen in non-dominant (right) hemisphere lesions and the head may be rotated and side flexed toward the unaffected side. The weak limbs of the affected side may cease to “belong” to the patient as they effectively disappear from the perceived body image. These limbs may be at considerable risk of physical trauma by wheelchairs, cot-sides and other such pieces of equipment. Patients may have great difficulty in turning to visualise anything appearing from the affected side including people trying to initiate conversation. This must be taken into account when assessing the extent of the perceptual deficit. Visuospatial inattention may exist in the presence of homonymous hemianopia, but the two may exist separately.
Homonymous hemianopia
This constitutes the loss of half of the visual field of each eye. The retinas on the same side as the lesion are affected and so the patient fails to see the image from the opposite side of the visual field. Thus, with a right hemisphere stroke the right half of each retina does not see, creating loss of vision to the left.
When associated with inattention also, the effect is a profound inability to see or perceive their affected side. This may be tested by asking the patient to look at your nose while you steady their head. You then bring an object such as a pen into the unaffected visual field from the periphery, asking the patient to indicate when they see it without looking directly at it. Repeat this process on the affected side and compare the position that the object was visualised in that field. This will allow you to establish whether a visual deficit exists.
Intact sensation is required for normal movement and function. Generally this is best tested in supine lying and is often part of the initial ward assessment. Having established the major abnormalities and their implications for treatment it is not necessary to repeatedly retest these, but an overall awareness is recommended.
Tactile awareness
Light touch and deep pressure may be assessed by placing your hand on the patient’s skin working from proximal to distal. If the patient cannot detect firm stroking stimuli (i.e. gross touch) then assessing light touch is usually pointless. In that case try tapping on bony points such as the knee cap and the elbow. If the patient is aware of firm touch then progress to light stroking with the finger tips or cotton wool to establish the degree of fine sensory loss. It is important to also test both sides simultaneously to establish whether the patient can perceive touch on both sides simultaneously.
Proprioception
Proprioception describes the perception of both joint movement and joint position. Joint motion awareness may be tested by supporting the limb and passively moving one joint at a time while the patient closes their eyes. Ask them first to report whether the limb is “still” or “moving” and if they are aware of the movement then to localise to which joint. Alternatively hold the thumb or great toe, tell the patient that flexion is “down” and extension is “up” and to report which direction they perceive the movement to be.
Joint position sense may be tested by asking the patient to copy the posture achieved passively by the tester on the affected side, with the limbs of the unaffected side. The patient should have their eyes closed during the test.
A useful global test of proprioception in the upper limb involves asking the patient to grasp the thumb of the affected hand with the un-affected hand while the tester moves the affected arm into different positions (with care of the shoulder). Initially the patient can look to see where the limb is to allow an appropriate understanding of the test, but they should have their eyes closed during the test.
Assessing passive joint range of movement is important as many people (and particularly older patients) suffer stiffness and loss of joint range through previous injury or other musculoskeletal problems. This may have implications for the rehabilitation strategies which may be attempted.
Limbs should be handled carefully, slowly and only moved within normal anatomical range. Particular care must be taken when moving the limbs of patients who present with very low tone and with a lack of sensation. Generally it is not necessary to measure the exact ROM in all joints, but commonly an estimate of the extent of the lack of movement is made i.e. half or quarter range.
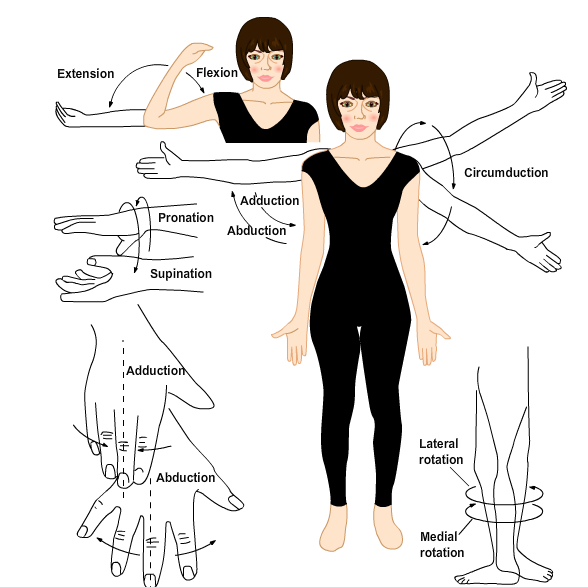
The diagram demonstrates: extension and flexion as movements of the elbow; circumduction, adduction and abduction as movements of the upper arm; pronation and supination in rotation of the wrist; adduction and abduction in the spreading and closing of fingers; and lateral or medial rotation as movements of the lower leg.
Active movement/power
Describe the patterns of active i.e. voluntary movement available on the affected side. Some use the Oxford (MRC) Scale:
0 No movement
1 Flickers of movement
2 Movement but only with gravity counterbalanced
3 Movement against gravity
4 Movement against resistance
5 Normal movement
Wade, D.T. 1992. Measurement in neurological rehabilitation. Oxford University Press.
Following a stroke patients may present with abnormal tone which may be decreased (hypotonus), increased (hypertonus) or a combination of the two. A combination of the two occurs where there is increased tone in one muscle group and decreased tone in another.
Tone may be increased temporarily by pain, discomfort, anxiety, effort and certain body positions.
Hypotonus
Low-toned muscles are floppy and sag away from their bony connections leaving the associated joints unsupported and unstable.
Low-toned limbs feel heavy and drop against gravity when handled if insufficient support is given. The muscle groups will feel flabby to handle and little or no resistance will be felt through the range of the movement. Great care must be taken to ensure adequate support of joints throughout their range of movement to prevent trauma, particularly to the shoulder.
Hypertonus
High-toned muscles are tense and bulky, with tendons visible beneath the skin. Joints spanned by high tone muscles will assume a shortened position rendering the patient unable to relax.
High-toned muscles will resist movement and feel tight.
Tone diagrams: these findings may be recorded using a tone diagram where high-tone muscles are shown with a (+) and low-tone muscles with a (-).
Base of support (BOS) is the surface area supporting the body or body part. A larger base of support e.g. lying down, allows greater muscle relaxation and therefore decreases muscle tone. A smaller base of support e.g. standing up, encourages more activity in muscles and therefore increases muscle tone.
By manipulating a patient’s base of support it is possible to alter their presenting patterns of muscle tone.