The outcome of Connie’s swallow screen is that she coughed when given teaspoons of water. This indicates that she that she requires a more detailed swallowing assessment from the Speech and Language Therapist, and should remain nil by mouth until this is completed. The staff involved in Connie’s care are also aware of the Standard Operating Procedure in their health board relating to nil by mouth status.
There are 5 key areas to consider that will be discussed in the coming pages:
Connie is 67 years old, widowed and lives alone. Today she was found collapsed at home by her daughter.
Her daughter called 999 as Connie was FAST positive and stroke was suspected. On arrival at the hospital she was examined and a CT of her brain was ordered.
She has now had a CT scan which has confirmed a cerebral infarct.
Connie also has a history of heart failure and atrial fibrillation.
Part 1 – Early Assessment
In this section, you will be working through a number of tasks to ensure that Connie’s food, fluid and nutrition needs are assessed and identified. This will ensure that Connie receives the best possible start to her stroke care, minimises her complications and gives her the optimal chance of recovery. Swallow screening should be carried out on 100% of stroke patients within 4 hours of admission (Scottish Stroke Care Audit Standard, available at: strokeaudit.scot.nhs.uk/Quality/Scottish_Stroke_Care_Standards.html)
Part 2 – Early Management
In this section, you will go on to assess Connie’s swallowing ability, her nutrition and fluid needs in detail. This includes the swallow screening procedure, assessment of her nutritional needs, the introduction of specialised diets and the International Dysphagia Diet Standardisation Framework and the management of the environmental factors along with methods that can be used to increase and supplement Connie’s food and fluid intake.
On completion of this module you should have a critical understanding of the importance of achieving a patient’s optimal nutritional status to support their recovery following stroke. This will include addressing the challenges of achieving optimal nutritional status in patients with dysphagia.
You will learn:
The procedures for screening patients in the acute phase of stroke to determine nutritional risk, hydration and the presence of a swallowing difficulty.
Management of patients with swallowing difficulties post stroke.
Management of non-oral feeding methods used post stroke: nasogastric (NG) tube and gastrostomy tube feeding
Management of hydration following stroke.
Oral health conditions and maintenance of optimal oral health following stroke.
Ethical issues around oral, non-oral feeding and hydration post stroke.
Importance of involving patients and families in decision-making following stroke.
Group Lead: Gillian Capriotti, Senior Speech & Language Therapist, NHS Greater Glasgow & Clyde
Group Members: Morag Ogilvie, Specialist Dietitian, NHS Forth Valley Amy Anderson, Staff Nurse, NHS Forth Valley Sheena Borthwick, Clinical Specialist Speech & Language Therapist, NHS Lothian Marion Ireland, Specialist Dietitian, NHS Lothian Ann McCrimmon, Nutrition Nurse Specialist, NHS Greater Glasgow & Clyde
Critical Readers: Prof Martin Dennis, Professor of Stroke Medicine, University of Edinburgh Gillian Currie, Stroke Training Coordinator, CHSS Jacqualin Barron, Senior Dietitian, NHS Highland Lynn Reid, Lead Training Coordinator, CHSS Hazel Hamilton, Stroke Coordinator, NHS Highland Anne Marie Irving, Senior Speech and Language Therapist, NHS Forth Valley
On completion of this module you should have a critical understanding of the importance of achieving a patient’s optimal nutritional status to support their recovery following stroke. This will include addressing the challenges of achieving optimal nutritional status in patients with dysphagia.
The answers to all the test questions are contained within the module. This information may be provided in the ‘Additional Information’ boxes on some of the pages.
Following surgery Maisie is recovering in HDU and her condition has improved significantly. Her GCS has returned to 14 (E4 V4 M6) and it is hoped she will return to the acute stroke unit in the next couple of days for rehabilitation.
Updated evidence no longer supports an age cut-off for surgery (NICE, 2019)
Is within 48 hrs of symptom onset
Her CT scan shows severe MCA territory infarct with massive cerebral oedema, with a score above 15 on the National Institutes of Health Stroke Scale (NIHSS) stroke severity score.
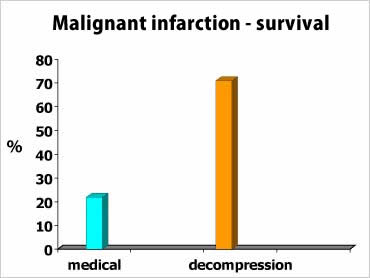
Patients with stroke involving the MCA territory and complicated massive cerebral oedema comprise a small proportion (2 – 8%) of the overall number of patients with stroke. Younger patients tend to be over represented in this group and the untreated mortality is very high (up to 80%).
Pooled analysis of the data from randomised controlled trials (RCT) of hemicraniectomy for malignant MCA infarction found significantly reduced mortality with hemicraniectomy. Malignant middle cerebral artery (MCA) infarction is a devastating condition leading to early death in nearly 80% of cases due to the rapid rise of intracranial pressure despite maximum medical management of the ischaemic brain oedema.