Background information on the Glasgow coma scale (GCS)
The Glasgow coma scale (GCS) is a neurological scale which aims to give a reliable, objective way of recording the conscious state of a person, for initial as well as continuing assessment. Glasgow Coma Scale (GCS)
Three types of response are measured:
Best motor response – maximum score of 6
Best verbal response – maximum score of 5
Eye opening – maximum score of 4
The lowest score for each category is 1, therefore the lowest score possible is 3 (= no response to pain + no verbalisation + no eye opening). A healthy person will score 15/15.
A patient with a GCS less than or equal to 8 requires the early involvement of an anaesthetist or critical care physician to provide appropriate airway management.
Reduction in motor score by one or an overall deterioration of two is significant and should be reported
Differences in GCS scores of two or more have been reported on the same patients by different practitioners. This reinforces that clinical decisions should not be solely based upon GCS but be used as a component of neurological function.
Glasgow coma scale:
Score
Eye opening
Spontaneous – Open before stimulus(+4)
To Sound – After spoken request (+3)
To Pressure – After fingertip stimulus (+2)
None – No opening at any time, no interfering factor (+1)
Closed by local factor – (NT)
Verbal response
Oriented – Correctly gives name, place, and date (+5)
Confused – Not orientated but communicates coherently (+4)
Words – Intelligible single words (+3)
Sounds – Only moan/groans (+2)
None – No audible response, no interfering factor (+1)
Non-testable – Factor interfering with communication (NT)
Motor response
Obeys Commands – 2-part request (+6)
Localising – Brings hand above clavicle to stimulus on head/neck (+5)
Normal Flexion – Bends arm at elbow rapidly but features not predominantly abnormal (+4)
Abnormal flexion – Bends arm at elbow, features clearly predominantly abnormal (+3)
Extension – Extends arm at elbow (+2)
None – No movement in arms/legs, no interfering factor (+1)
Non-testable – Paralysed or other limiting factor (NT)
Maximum score
15
GCS assessment method updates-
Check: To check for any factors that might interfere with the assessment, for example stroke patients may have hemiparesis, dysphasia and hearing loss.
Observe: To see for spontaneous patient actions (e.g. eye opening).
Stimulate: Once it is decided that there is no spontaneous response then to stimulate and check for responses.
Rate: After the stimulation for various parameters the score is recorded and totalled to arrive at the GCS score. If the initial check identifies cannot be assessed appropriately, the rating is classified as “not testable” and recorded NT.
Health professionals use the aforementioned scale for the best eye opening response, the best motor response, and the best verbal response. Consideration is made for those with tracheostomy and endotracheal breathing tubes.
In this case it is expected that you will have learned and understood the following points:
To be able to recognise normal and abnormal respiratory rate, heart rate, temperature, oxygen saturation levels and an irregular heart rate suggestive of atrial fibrillation.
To be able to recognise the causes of abnormal respiratory rate, heart rate, temperature, oxygen saturation levels and atrial fibrillation.
To recognise what actions are needed when abnormalities of respiratory rate, heart rate, temperature, oxygen saturation levels have been identified
To understand the potential harm of these abnormal physiological parameters when left untreated.
A basic understanding of identifying and treating atrial fibrillation
Recognising the urgency of active intervention both in monitoring and treatment
Q. Why is atrial fibrillation particularly relevant in Stroke patients? Select Yes or No for each question below.
see view text alternative for more information on correct answers
Atrial Fibrillation strokes are more disabling and 1 in 5 experience recurrent strokes and are associated with high mortality rates (Alkhouli et al, 2018)
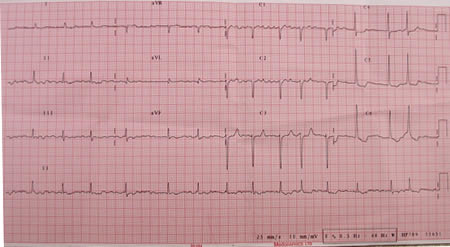
The following day Archie’s condition has generally improved but whilst taking a set of measurements you note that he has an irregular heart rate. As per NICE guidelines https://cks.nice.org.uk/atrial-fibrillation, an electrocardiogram (ECG) is arranged and the results show that he in atrial fibrillation (see ECG below).
Note – care must be taken when measuring heart rate in patients in atrial fibrillation. The most accurate readings will be achieved by either using a cardiac monitor or listening at the heart with a stethoscope and counting the heart rate. Taking the pulse rate using either an automated blood pressure cuff or counting the pulse at the wrist is not sufficiently reliable.
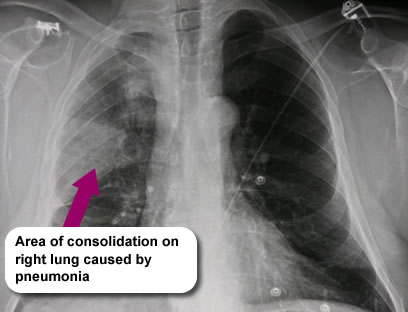
Following the doctor’s examination and initial investigations, Archie is diagnosed with pneumonia and has blood cultures taken. He is commenced on treatment with antibiotics and commenced on oxygen therapy, via nasal cannulae, to ensure oxygen saturation is maintained between 94-98% (British Thoracic Society 2017). Archie is also prescribed regular paracetamol to lower his temperature.
See Additional Information to find out how you should give oxygen accurately.
The doctor reviews Archie and is concerned about his raised temperature.
Select each of the crosses below to find out why you would be concerned about an increased temperature in the acute phase of stroke.
One principle of acute management is to keep temperature normal. This can be done with 48 hrs of regular paracetamol to bring the temperature down over this period. Review after 48hrs.
You call the on-call doctor who advises that you begin treatment with oxygen and repeat his observations after 30 minutes. At this point Archie is sweaty and restless and his observations are as below.
Q. Are Archie’s results normal? Select either normal or abnormal for each result below.
For more information on correct answers see view text alternative.
These test results indicate that further action is needed. In cases of acute hypoxaemia, treatment should be started with nasal cannulae (or a simple face mask, if nasal cannulae are not tolerated or not effective) with the flow rate adjusted to achieve a saturation of 94–98% (British Thoracic Society guideline for oxygen use in healthcare and emergency settings, 2017).
You carry out a swallow screening test with Archie which prompts some coughing. The video below shows how to carry out a swallow screening test.
As a result you recommend that Archie is nil by mouth (NBM) that he is referred for a Speech and Language Therapy assessment and has intravenous fluids in the meantime.
Animation showing the normal swallow and Archie’s swallow.