No!
For every 100 patients treated with stockings about three developed skins breaks associated with the stocking use. If you fit stockings to 35 patients you are likely to cause one skin break.
Pressure sore behind the knee where the rolled stockings has damaged the skin.

Results of CLOTS 1
Stockings do not reduce the risk of dying but do increase the risk of skin breaks.
(See the Research topic loop below for further information.)
Topic Loop:
Do stockings reduce the risk of DVT? No!
About 10% of patients treated with stockings developed proximal (above knee) DVTs. This was the same proportion as in the group without stockings.
CLOTS 1 – 30 day venous thromboembolism (VTE) outcomes
The differences in the % of patients developing a DVT or PE in the two groups were very small. This difference could easily have been due to chance. NS refers to ‘Not significant’ which reflects that the differences between the groups could be explained by chance alone.’
(See the Research topic loop below for further information.)
Topic Loop:
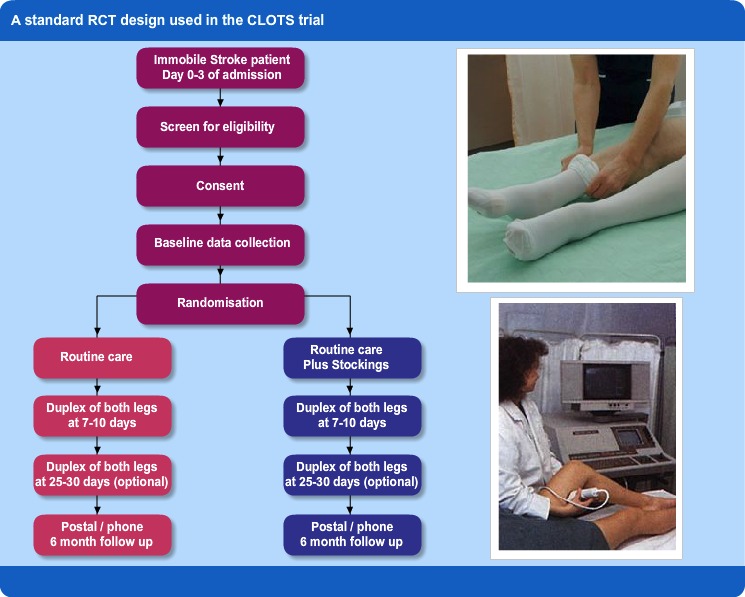
The CLOTS trial used a standard RCT design, see the ‘Research’ topic loop for more information.
Topic Loop:
To answer this question this multicentre randomised trial (see ‘Research’ topic loop at the bottom of the page) was set up to assess the effectiveness of stockings in stroke patients.
The trial was funded by the Medical Research Council (UK), Chief Scientist Office, Scottish Government, Chest Heart & Stroke Scotland and supported by the UK Stroke Research Network.




Between 2001 and 2009 over 2500 patients were enrolled in 64 UK hospitals. More details are available on the CLOTS website.
Topic Loop:
Stockings have been used for many years to reduce the risk of DVT in patients having surgery. Surgery patients:
- can be fitted with stockings before they are immobile
- are usually immobile for a short time
- many can manage their own stockings so they are not rolled down around their knees!
Stroke patients:
- cannot be fitted before they become immobile, so the DVT may already have formed
- are often immobile for weeks
- are less able to apply their own or ensure that they are not rolling down
- more often have peripheral vascular disease or diabetes which makes stockings riskier
Assessing the effectiveness of stockings in surgical patients provided strong evidence that they are effective. However it was unclear whether the evidence for effectiveness in surgical patients applied to medical patients and those with stroke. The HTA review recommended more research in medical patients, and specifically those with stroke so the following Research Question arose and needed to be addressed:
“Does the routine application of thigh-length graduated compression stockings (GCS) reduce the risk of proximal DVT in immobile stroke patients admitted to hospital?”
Topic Loops:
Neither prescribing heparin or applying stockings are correct courses of action for Brenda.
Why Brenda should not be given heparin:
| Guideline |
Description |
| SIGN 118 |
SIGN 118 guideline does not recommend anticoagulation: ‘Anticoagulant therapy in the first two weeks after ischaemic stroke can cause haemorrhagic stroke or haemorrhagic transformation of the ischaemic stroke and has no net benefit 1++” |
| NICE |
NICE guidelines [.pdf] do not recommend routine anticoagulation for patients with stroke: ‘Anticoagulation treatment should not be used routinely for the treatment of acute stroke’ |
| Cochrane review |
Cochrane review : A systematic review of all relevant trials indicates that whilst heparin will reduce the risk of DVT (mostly asymptomatic DVTs picked up only on scans) it will also increase the risk of serious bleeding. Patients treated with heparin do not have better overall outcomes than those without i.e. they have similar mortality and functional outcomes. |
(See the Evidence and Evidence based guidelines topic loops below for further information on the above.)
Highly selected patients who are judged to be at low risk of bleeding but much higher than average risk of DVT may be treated based on a clinician’s individual judgment.
For Brenda the issue is whether the heparin was written up following such an assessment or simply because the junior doctor was applying the protocol for non stroke patients to her – in error!
Why Brenda should not have stockings applied:
| Guideline |
Description |
| SIGN 118 |
The SIGN 118 guideline states: ‘Above-knee graduated elastic compression stockings to reduce the risk of deep vein thrombosis after acute stroke are not recommended” Grade A, Level 1++’ |
| NICE |
NICE guideline [.pdf] on prevention of venous thromboembolism (Jan 2010) states: “Do not offer anti-embolism stockings for VTE prophylaxis to patients who are admitted for stroke.” |

Brenda
 Brenda is 66 years old and is married with three young grandchildren. She was previously well except for having high blood pressure, being overweight and being an ex-smoker.
Brenda is 66 years old and is married with three young grandchildren. She was previously well except for having high blood pressure, being overweight and being an ex-smoker.
Yesterday she was admitted to the medical assessment ward at 9pm with a left hemisphere stroke causing aphasia and right side weakness – she presented too late to benefit from thrombolysis. On admission she was unable to walk or talk and unable to answer even simple questions. The CT scan excluded intracerebral haemorrhage.
She was transferred up to the stroke unit in the morning of the following day (in line with Scottish Stroke Care Standards 2016)
She was transferred up to the stroke unit in the morning of the following day (in line with Scottish Stroke care standards (2016) and Local Delivery Plans (LDP) – see the Clinical standards topic loop below for further information). She received 300mg of aspirin orally after she passed her swallow screen in the assessment unit and has been prescribed heparin and anti-embolism stockings (e.g. TED) by the doctors in the assessment ward but these have not yet been started.
You are the nurse in charge of the stroke unit. What will you do with respect of these prescriptions?
Topic Loop:
You can contribute to service improvement by:
- Working to evidence based standards of care
- Participating in collecting data to measure performance against standards
- Taking note of local services performance and play a part in improving it
- Joining MCN or national groups to take forward the agenda
- Facilitating the participation of your patients in well designed research projects such as randomised trials
To answer the questions in the quiz below you will need to have gone through the 6 topic loops on the right.
Q. Which of the following statements are true? Select true or false for each of the options listed below.
Topic Loops:
Each of the components featured in the learning points fit together into the quality cycle as shown below.
Topic Loops: