Discharge
Jason’s blood pressure reduction medication is commenced 4 days post stroke (see Topic Loop below for further information). He has had no further seizures and is discharged home with a follow up appointment with the stroke liaison nurse planned for a week later. Jason has also been referred to the specialist alcohol and drugs services who will liaise with him and his partner Suzanne on discharge home.
Follow up
The following week, the stroke liaison nurse visits Jason at home. She measures his blood pressure at 140/87. This is still too high so she advises him to see the practice nurse to have it repeated the following week. She also readdresses the lifestyle risk factors which previously were at the preparation stage of the ‘Readiness to change’ model prior to his discharge to see how he is progressing.
Alcohol – Jason is still planning to reduce his alcohol intake following his 40th birthday which is in one months time. The stroke liaison nurse has some concerns that this might be difficult for Jason as Suzanne reports he has been continuing to drink.
Recreational drugs – Regarding his recreational drug use Jason says “I’ve deleted the number of my dealer from my mobile phone and haven’t seen him since I have been home and I have chucked away all the cocaine that was in the house.”
Topic Loops:
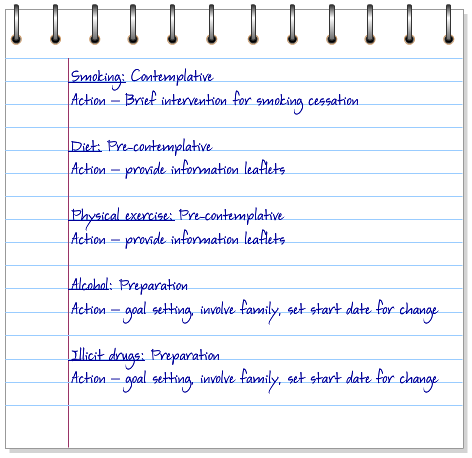
You have identified that Jason is at the Preparation stage for making changes for alcohol and recreational drugs.
As a health professional what actions would you take at this stage? Select True or False for each of the following:
For further information on SMART goals see behaviour change Topic Loop below.
Topic Loop:
You have identified that Jason is at the Contemplative stage for making changes for smoking.
As a health professional what actions would you take at this stage? Select true or false to the statements below.
CHSS supports the Charter for a smoke free generation in Scotland by 2034 to protect young people and support positive health choices.
In order to support Jason with his plans and continue to encourage and motivate him, we need to look at each lifestyle risk factor and the stage of change he is currently at. You have identified that Jason is at the Pre-contemplative stage for making changes to his diet and exercise.
What actions would you take at this stage? Select true or false to the statements below.
Later that afternoon the nurse has a meeting with Jason and Suzanne. She asks Jason about his lifestyle and they identify smoking, excessive alcohol, illicit drugs, low physical activity and poor diet as key areas which need addressing. The nurse now needs to assess Jason’s readiness to change.
Jason makes the following statements about his smoking, recreational drugs, physical activity and diet habits. As Jason is still in hospital and this is the first time he has discussed this, he hasn’t had time to make any actual changes yet. Using the Prochaska and DiClimente model (see behaviour change Topic Loop for more information) decide which of the first 3 stages of change Jason is at for each lifestyle risk.
Topic Loop:
Jason is feeling agitated about being in a ward with “all these old folk” and you overhear him telling the man in the next bed that he doesn’t understand what all the fuss is about; his pal’s dad smoked and drank all his life and lived into his 80’s. He says how much he misses drinking alcohol and smoking (for further information see Topic Loops below). You are concerned that Jason does not recognise the impact of his lifestyle behaviour on his health.
Later that evening Jason has a seizure which is witnessed by 2 of the nursing staff. The doctor tells Jason that seizures are quite common after a stroke due to a bleed and that it is also likely to be related to alcohol withdrawal.
Jason admits to drinking 5 pints of beer a day. Set the drinks calculator below to see how many units of alcohol a day Jason is taking (the beer that Jason drinks is 5% alcohol)
Click here to open the DrinkAware calculator (opens in a separate browser tab)
The following morning his partner Suzanne visits him and notices that he seems unusually quiet and withdrawn. He tells her that he is worried that he is going to die.
Topic Loops:
What we know about Jason so far is that:
- Jason has had a haemorrhagic stroke which has been confirmed by a CT scan
- No rare causes were identified
It is 8 hours since Jason’s partner Suzanne phoned NHS 24 and Jason has now been admitted to the stroke unit.
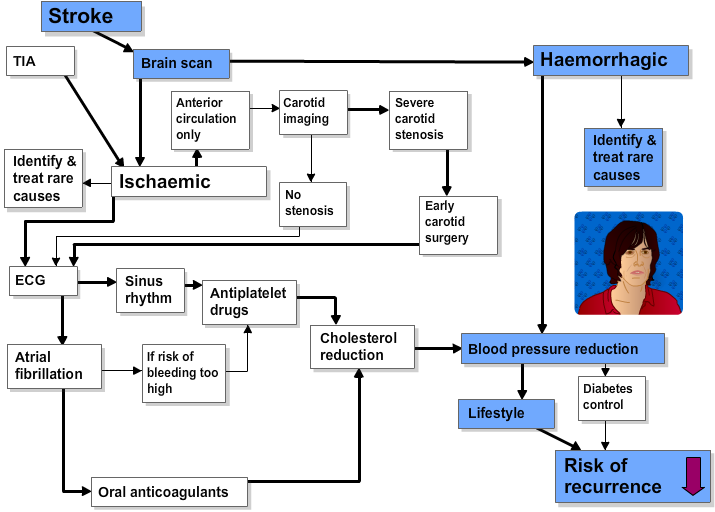
Q. Which of the following medications should Jason now be prescribed?
Blood tests and other investigations are carried out to screen for common risk factors and unusual causes of stroke.
| Test |
Results |
| FBC |
Hb 128g/l (NR 130-180), MCV 105fl (NR 78-98), WBC 4.5×109/l (NR 4-11), Plat 120 (NR 150-350) |
| ESR |
10mm/hr (NR 1-10) |
| U&Es |
Na 129mmol/l (NR 135-145), K 4.9mmol/l (NR 3.6-5.0), urea 2.3mmol/l (NR 2.5-6.6), creat 78 umol/L (NR 60-120) |
| LFTs |
Bilirubin 21(NR 3-16 umol/L) ALT 123U/l (NR 10-50) ALP 176U/l(NR 40-125) GGT 110U/l (NR 10-55) |
| Prothrombin time ratio |
1.6 (NR 0.9-1.3) |
| Blood sugar |
4.5mmol/l (NR 3.2- 5.5) |
| Cholesterol |
5.6mmol/l (NR 2.5-5.5) |
| C Reactive protein |
< 3mg/l (NR 0-10) |
| ECG |
sinus rhythm 72/min, normal |
| Echocardiogram |
normal, no vegetations |
| Blood cultures |
no growth |
The CT scan shows a haemorrhage in the right internal capsule and excludes alternative non stroke diagnoses. Jason is admitted to the NuYu stroke unit.
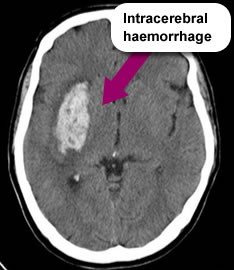
So, he has macrocytosis (raised MCV – large red cells), a lowish platelet count, low sodium and urea, abnormal LFTs and a slightly high INR (abnormal clotting) which all fit with a history of excessive alcohol intake perhaps causing a degree of liver disease. He has had a haemorrhagic stroke, potential causes and risk facors include:
- High blood pressure (contributed to by alcohol)
- Cocaine abuse
- Abnormal coagulation
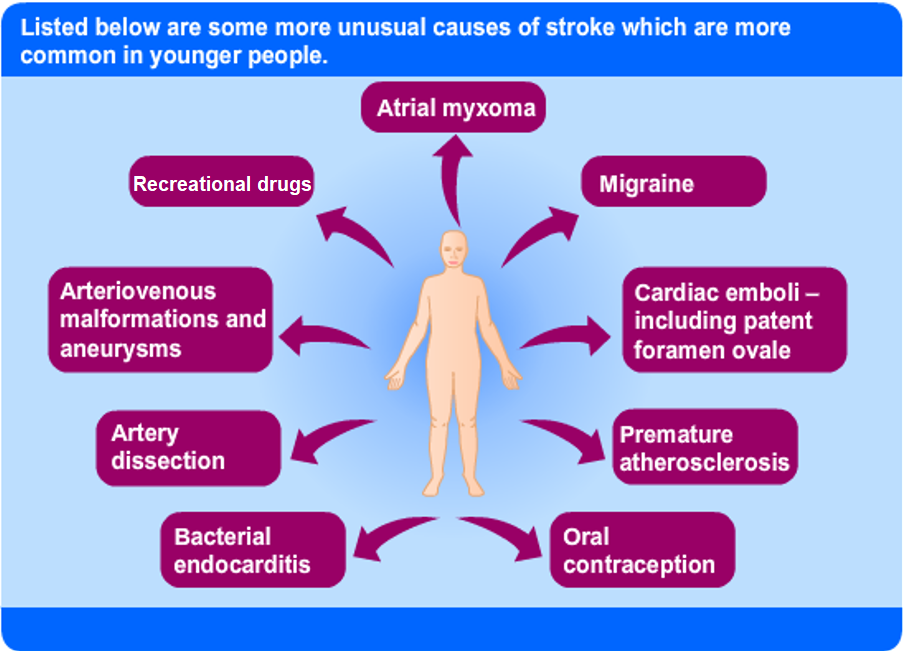
There are some more unusual causes of stroke which are more common in younger people (also see Topic Loops below).
Topic loops: