An ambulance arrives and takes Iain to A&E where he is assessed by a doctor who takes his medical history.
Iain does not have any headache or sickness, his symptoms are improving but he still has some weakness in his left hand.
An ambulance arrives and takes Iain to A&E where he is assessed by a doctor who takes his medical history.
Iain does not have any headache or sickness, his symptoms are improving but he still has some weakness in his left hand.


Iain is a retired man aged 75. Whilst on the golf course Iain suddenly develops a weakness of his left arm, drops his club and he can’t pick it up. Fortunately he is playing golf with a retired Doctor who recognises the symptoms of stroke.
On discharge from hospital, therapy and support will continue to address her ongoing needs. Isa has a number of follow-up appointments in her diary.

Isa has a BMI of 28 and she also has high cholesterol.
When the stroke liaison nurse talks to Isa on the ward, Isa tells her that she has a good diet as she doesn’t have a sweet tooth and never eats puddings or cakes. When asked about what she has at mealtimes, Isa then reveals that she goes to the bingo several days a week where she has the daily special. She particularly likes the ‘fish tea’ as it is only £3.00! For further information see Topic Loops below.

The liaison nurse sees this as an opportunity for a brief intervention and shows Isa the eatwell plate.
Isa had thought because it was white fish it was healthy but hadn’t accounted for the batter coating or the chips!
As a result of the brief intervention, Isa has decided she would like more information about healthy eating. She is going home tomorrow, so the liaison nurse arranges for Isa to see the dietitian when she is at the day hospital for further advice.
Four main strategies have been devised from the feedback at the MDT meeting regarding Isa’s medication management. Go through the slides to find out more on the pie chart segments.

For further information on medication adherence see Topic Loop below.
Following the diagram below we know that:
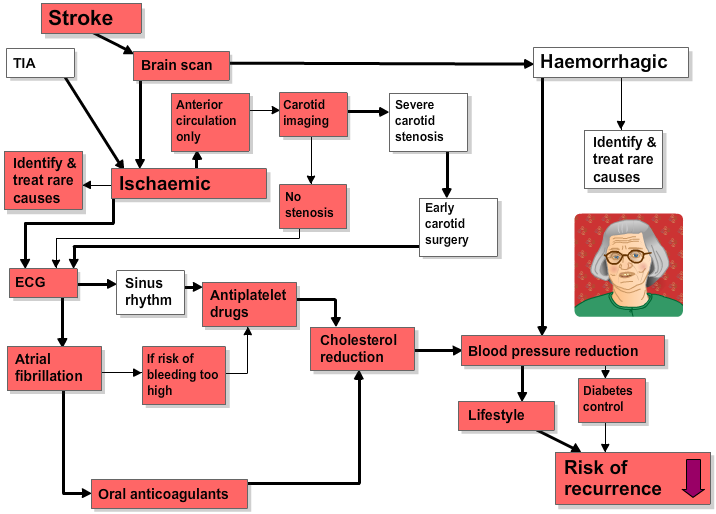
Although it seems likely that Isa’s ischaemic stroke is due to embolism from her atrial fibrillation she has mild anaemia and a raised erythrocyte sedimentation rate (ESR) which raises the possibility of rarer causes such as:
See Topic Loops below for further information on these.
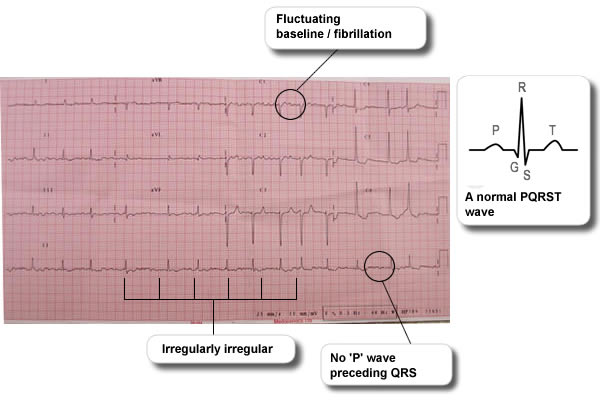
Isa’s electrocardiogram (ECG) confirms that she has atrial fibrillation (see ECG below). For further information see Topic Loops below.
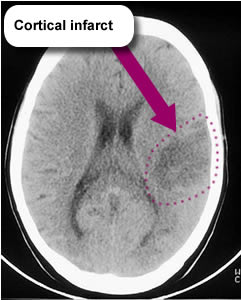
Isa’s CT brain scan below shows a moderate sized cortical infarct in the left hemisphere.
Isa’s carotid duplex shows minor atheroma only.