Meet Evelyn
Evelyn is 67 years old and married to Tom. She retired from her cleaning job at the local primary school almost a year ago. Evelyn has borderline (stage 1) hypertension. She has been trying to modify her lifestyle since this was diagnosed. She is not on any medication for her blood pressure.
Please enable JavaScript in your browser to see this interactive content.
There are a variety of risk estimation tools available. The ASSIGN Score is the one validated and recommended for use in Scotland.
Some of the others are:
- QRISK, which is recommended by NICE
- Joint British Societies (JBS) 2 and 3
JBS guidelines on prevention of cardiovascular disease in clinical practice
JBS 3 Risk Calculator
Exclusions for using any of the RISK calculators:
- People with established cardiovascular disease
- People with type II diabetes
- People with target organ damage ( i.e. LVH)
- People with chronic kidney disease
- People with familial hyperlipidaemia
People with the above conditions are considered high risk for CVD and so will be medically managed for their hypertension. Therefore, the above risk calculators are not valid as they underestimate the CVD risk.
Paul returns to the Practice Nurse after carrying out home monitoring for a week.
Please enable JavaScript in your browser to see this interactive content.
Patient information about left ventricular hypertrophy: Blood Pressure UK (Enlarged Heart LVH)
The normal procedure in Paul’s General Practice is for people to have 24 hour BP monitors fitted. However, this would mean Paul would be unable to drive while the monitor is in place, as his arm has to be kept straight when the cuff inflates.
- Paul explains to the Practice Nurse that this will not be possible over the next few weeks because he is required to travel with his job. It is important that all care is person centred and so the practice nurse instead arranges for him to do home blood pressure monitoring.
Basics instructions for people doing home monitoring:
- Two consecutive seated measurements, at least 1 minute apart
- Blood pressure is recorded twice daily (ideally morning and evening)
- Record for at least 4 days and preferably for a week
- Measurements on the first day are discarded and average value of all remaining is used for each blood pressure recording
N.B There is a home blood pressure monitor that NICE recommend for people known to have atrial fibrillation: it is called WatchBP. NICE Guidelines on Atrial Fibrillation
When fitting a home blood pressure monitor, ensure that:
- The pulse is regular
- The cuff is the correct size
- The person is able to operate the machine
Paul’s blood pressure is elevated at the appointment with the practice nurse. As a result, the practice nurse will arrange the following tests:
Dipstick testing of urine for proteinuria
The presence of protein in urine identifies patients with kidney damage, but does not distinguish between patients who have renal disease and secondary hypertension and those in whom kidney damage is due to essential hypertension. (Ref: NICE Clinical Guideline 73)
Blood tests – U&Es, cholesterol and glucose levels
U&E’s are measured to assess kidney function and to exclude renal disease as a cause or consequence of Hypertension. Sodium and potassium levels are checked to exclude hypertension resulting from adrenal disease. Glucose and cholesterol profiles are used to assess cardiovascular risk. (Ref. NICE guidelines 17, 87)
12 lead electrocardiogram (ECG)
An ECG can reveal a person’s heart rate, heart rhythm and highlight any conduction abnormalities. It can show left ventricular size and any highlight damage to specific areas of the heart muscle. In hypertension the presence of left ventricualr hypertrophy (LVH) can be an indicator of target organ damage. If the ECG is suggestive of LVH, an echocardiogram must be performed to either confirm or refute the presence of LVH suggested by the ECG. In some people, particularly slim or athletic individuals, the ECG may suggest LVH but on echocardiogram the left ventricle size will be normal. However, If LVH is present on the echocardiogram then the person must be treated life-long for hypertension, irrespective of their cardiocavular risk calculator score.
Fundoscopy
This is an examination of the eye to detect hypertensive retinopathy, which is a result of untreated hypertension. Most people with hypertensive retinopathy do not have symptoms until late in the disease. Symptoms may include: double vision; dim vision; loss of vision; or headaches. The only treatment for hypertensive retinopathy is good blood pressure control.
Paul has made an appointment to see his GP to discuss an abnormal blood pressure result, taken at his local gym.
Please enable JavaScript in your browser to see this interactive content.

Meet Paul

Paul is a 43 year old man who works as an architect. He lives with his partner and two young children. He keeps fit by cycling and running, and he enjoys days out to the park with his children. Paul has recently gone to join a new local gym, where he undergoes a health check prior to being admitted as a member.
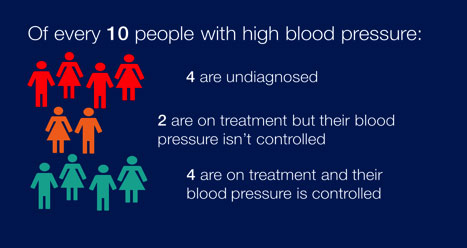
All people over 16 years should have their BP checked every 5 years to identify those at risk and more frequently if BP is high normal (130-139/85-89mmHg). The recognition and treatment of people with hypertension is currently sub-optimal.
For all people with hypertension cardiovascular risk should be assessed and managed. The presence of other risk factors (or cardiovascular disease) also increases the risk of morbidity and mortality, and the need to lower blood pressure. (See the HEARTe module Primary Prevention of Heart Disease for more information.)
RISK FACTORS TABLE
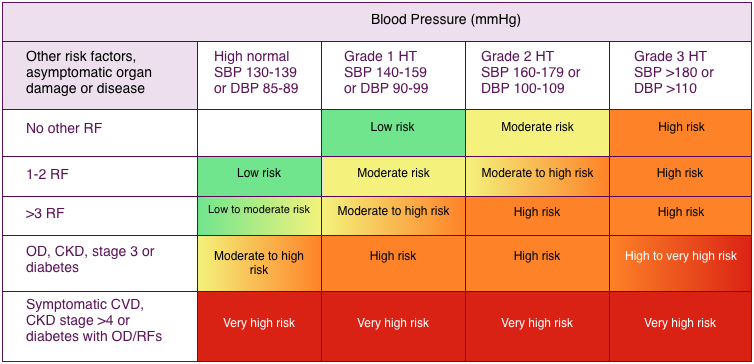
BP = blood pressure; CKD = chronic kidney disease; CV = cardiovascular; CVD = cardiovascular disease; DBP = diastolic blood pressure; HT = hypertension; OD = organ damage; RF = risk factor; SBP = systolic blood pressure.
Figure 1 Stratification of total CV risk in categories of low, moderate, high and very high risk according to SBP and DBP and prevalence of RFs, asymptomatic OD, diabetes, CKD stage or symptomatic CVD. Subjects with a high normal office but a raised out-of-office BP (masked hypertension) have a CV risk in the hypertension range. Subjects with a high office BP but normal out-of-office BP (white coat hypertension), particularly if there is no diabetes, OD, CVD or CKD, have lower risk than sustained hypertension for the same office BP. (Ref. Journal of Hypertension).
It is important to provide information on stopping tobacco smoking to lower cardiovascular risk and moderating alcohol, salt and caffeine consumption to lower BP. Health professionals should also offer advice on weight loss (if appropriate), healthy diet, and regular exercise. Public Health England estimated that if, over 10 years, England achieved a 15% increase in the proportion of adults on treatment controlling their blood pressure to 140/90mmHg or below, £120m would be saved. (Ref: Public Health England (2014) High Blood Pressure: data guidance and health service planning.)