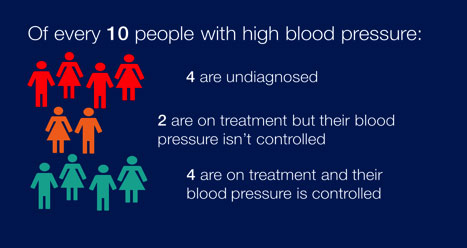
All people over 16 years should have their BP checked every 5 years to identify those at risk and more frequently if BP is high normal (130-139/85-89mmHg). The recognition and treatment of people with hypertension is currently sub-optimal.
For all people with hypertension cardiovascular risk should be assessed and managed. The presence of other risk factors (or cardiovascular disease) also increases the risk of morbidity and mortality, and the need to lower blood pressure. (See the HEARTe module Primary Prevention of Heart Disease for more information.)
RISK FACTORS TABLE
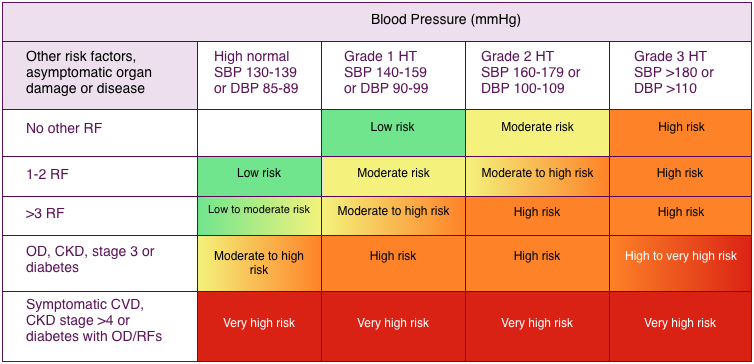
BP = blood pressure; CKD = chronic kidney disease; CV = cardiovascular; CVD = cardiovascular disease; DBP = diastolic blood pressure; HT = hypertension; OD = organ damage; RF = risk factor; SBP = systolic blood pressure.
It is important to provide information on stopping tobacco smoking to lower cardiovascular risk and moderating alcohol, salt and caffeine consumption to lower BP. Health professionals should also offer advice on weight loss (if appropriate), healthy diet, and regular exercise. Public Health England estimated that if, over 10 years, England achieved a 15% increase in the proportion of adults on treatment controlling their blood pressure to 140/90mmHg or below, £120m would be saved. (Ref: Public Health England (2014) High Blood Pressure: data guidance and health service planning.)
| Blood Pressure (mmHg) | ||||
| Other risk factors, asymptomatic organ damage or disease | High normal SBP 130-139 or DBP 85-89 | Grade 1 HT SBP 140-159 or DBP 90-99 | Grade 2 HT SBP 160-179 or DBP 100-109 | Grade 3 HT SBP >180 or DBP >110 |
| No other RF | Low risk | Moderate risk | High risk | |
| 1-2 RF | Low risk | Moderate risk | Moderate to high risk | High risk |
| >3 RF | Low to moderate risk | Moderate to high risk | High risk | High risk |
| OD, CKD, stage 3 or diabetes | Moderate to high risk | High risk | High risk | High to very high risk |
| Symptomatic CVD, CKD stage >4 or diabetes with OD/RFs | Very high risk | Very high risk | Very high risk | Very high risk |
Pulse point
What if BP is very high on assessment?
- Consider hospital admission if:
- BP is 220/120 mmHg or higher.
- BP is 180/110 mmHg or higher with signs of accelerated (malignant) hypertension (papilloedema and/or retinal haemorrhage).
- Start antihypertensives immediately if no signs of accelerated hypertension and:
- Systolic BP is 180 mmHg or higher, or
- Diastolic BP is 110 mmHg or higher.
(Ref: The European Society of Hypertension (ESH) and European Society of Cardiology (ESC) (2013) ESH/ESC Guidelines for the management of arterial hypertension. J Hypertens 31:1281–1357 DOI:10.1097/01.hjh.0000431740.32696.cc)
Page last reviewed: 17 Sep 2020